Total thyroidectomy is the removal of the entire thyroid gland.
The reasons for total thyroidectomy
The reasons a total thyroidectomy may be required include:
1. Thyroid enlargement
This is also known as a “goitre”. A goitre may cause symptoms of obstruction to swallowing, breathing, speaking, a constant cough, or neck discomfort. Occasionally a goitre does not cause any symptoms despite being very large.
2. Thyroid overactivity
An overactive thyroid is a condition known as hyperthyroidism. There are numerous causes of this condition, with one of the most known called Graves’ disease (named after the doctor who discovered the condition). Medication is usually able to control excessive thyroid hormone levels, but when other types of control are less effective, or where cardiac drugs produce thyroid overactivity but are beneficial for control cardiac rhythm (amiodarone), a thyroidectomy may be necessary.
3. Suspicion of thyroid cancer
4. Painful thyroid conditions
Thyroiditis is where the thyroid gland becomes inflamed. This is usually treatment with medications. Rarely it does not settle with time or has not responded to treatment or the side effects of medical treatment are unacceptable.
5. Benign thyroid conditions
These may need repeated investigation such as needle biopsy over time, are proving a source of anxiety and inconvenience for the patient
6. Definitive treatment with one operation
A condition which is mainly on one side of the thyroid but which is very likely to develop within a short time on the other side as well. Most patients in this situation prefer to have only one operation, as repeat surgery carries a slightly higher risk of complications.
There may be one or more factors that are important in any one patient. Every patient will react to their own illness in a different way so we use this list as a guide to making the decision about whether surgery is necessary and how much surgery is needed.
There may be one or more factors that are important in any one patient. Every patient will react to their own illness in a different way so we use this list as a guide to making the decision about whether surgery is necessary and how much surgery is needed.
What are the complications that can happen with any operation?
When patients undergo surgery there is a risk of having a heart attack or stroke, of developing kidney or lung failure. Generally these conditions are more likely if there is already evidence of a pre-existing illness, which is why your past history is noted in detail. If you have forgotten some part of the history, you can ring Dr Yeung’s rooms to fill in any gaps.
We take precautions with any major operation to minimise the risk of blood clots forming in the legs and pelvic veins. If these travel to the lungs they can occasionally be life threatening. You must make sure that if you or your family have a blood clot history, or if you have had leg immobilisation prior to surgery to let Dr Yeung know. All operations carry a risk of infection. The risk of infection is greater if you need to stay longer, have a long complex procedure, or have a depressed immune system, or other medical problems like diabetes.
Complications specific to thyroid surgery
Voice Complications
The larynx (the organ for speaking) lies just above the thyroid and there are nerves (recurrent laryngeal nerve) to make the vocal cords move for speech, to avoid food going “down the wrong way” and for coughing which run very close to the thyroid from above and below. It is important to avoid injury to these nerves during thyroid surgery. We may check the vocal cord function before or after your operation with a flexible telescope through the nose (nasendoscopy).
During surgery, Dr Yeung uses a nerve monitoring device – this allows her to confirm that the recurrent laryngeal nerve has been identified and is working during the operation. Temporary hoarseness affects about 10% of patients but is due to nerve damage in only half. Wound swelling, and vocal cord bruising from the anaesthetic tube are other causes. The external branch of the superior laryngeal nerve is another nerve encountered during thyroid surgery. It is responsible for voice pitch and projection. This nerve is usually identified and preserved during surgery. It may also be confirmed with the use of the nerve monitoring device. Permanent paralysis of one recurrent laryngeal nerve is uncommon (about 0.5%) and the nerve may take up to 2 years to recover. Often the other vocal cord can be strengthened to do the work for both sides. Very rarely (mostly with advanced thyroid cancer) both nerves do not work and a tracheostomy (breathing tube in the neck) is necessary, in some cases permanently.
It is unusual for thyroid patients not to be able to use their voice at the same level as before. Voice weakness and voice fatigue (losing the voice after prolonged speaking) are common symptoms that usually improve over six months. This can be due to the upper nerve of the larynx being damaged, and this may affect up to 30% of patients but is usually mild. We recommend using the voice as much as is comfortable as the larynx muscles, like muscles in the arms and legs, recover better if they are being exercised. This exercise is not always popular with other family members! If your work involves a lot of speaking we may recommend “light voice duties” to help with recovery.
Thyroid Hormone Replacement
When the whole thyroid is removed, replacement of thyroid hormone (a chemical made in the thyroid and released into the blood stream) is necessary to remain healthy. This hormone is given in the form of thyroxine which is a tablet form of the same chemical that is called T4 in the blood test that you may have had recently. This hormone is needed to maintain important metabolic (a bit like the accelerator pedal in a car) function. Usually 100 to 150 mcg (ug or micrograms) per day is enough. We usually test this with a blood test 6 weeks after surgery and 6 – 12 monthly afterwards. The level is usually easy to maintain and the dose needed may gradually get less as you grow older.
The prescription is inexpensive and the tablets come in blister packs. We give various combinations of 50, 100, and 200 mcg tablets. The dose lasts a few days in the blood stream so missing a dose and catching up occasionally is not a problem. Most people get in to a routine of taking the tablet on getting up in the morning. Thyroxine is absorbed through the intestine and the absorption can be affected by binding to calcium in calcium tablets and vitamin supplements containing calcium. Milk and soy products have large amounts of calcium which can have this effect.
We advise taking thyroxine on an empty stomach half to one hour before any of these products are consumed. You should not adjust the dose according to how you feel as the effect of changing the dose is delayed. If you are forgetful, the chemist has a dispenser with the days of the week marked on it, so you can set out your weeks’ medication and take it regularly.
Parathyroid glands
The parathyroid glands are located on both sides of the neck, so an operation on one thyroid lobe usually puts only half these glands at risk. As a result, the problems described below are rarely experienced, unless you have already had one thyroid lobe removed, or we need to remove both thyroid lobes. Behind the thyroid there are four tiny glands only 5mm in length. These glands have the same blood supply as the thyroid, and even with very careful surgery, they can be injured.
If this happens then the important parathyroid hormone (PTH) may fall, leading to low levels of calcium in the blood. As calcium is an important mineral for bones, muscles and nerves, a fall in calcium can lead to a loss of bone substance or osteoporosis, although this is a long term complication. More immediately low calcium can cause numbness, cramps, and pins & needle symptoms. These are easily fixed by giving calcium either in tablet form, and to bring the level up if very low, a potent form of Vitamin D, Calcitriol. About 25% of patients have some form of fall in calcium after surgery to remove both lobes of the thyroid (total thyroidectomy). Patients who have had previous thyroid surgery or Graves’ disease are more susceptible. About 1 in 50 patients need long term calcium and Rocaltrol replacement, but are usually otherwise healthy.
There may be an increased risk of developing cataracts, so an eye check and measurement of bone strength may be needed. Vitamin D is not used in pregnancy and calcium tablets are large so not always popular with patients who have trouble with tablets. Chewable and dissolvable forms are available. Several serves of dairy food or calcium enriched food may substitute for some calcium tablets.
If we are worried about the health of one or more parathyroid glands we may implant them into the sternomastoid muscle (the large diagonal muscle on the front of the neck). Here they develop a new blood supply like a skin graft and work well after 6 weeks. If there is a temporary problem, this is usually better within 2-3 weeks but sometimes takes 6-12 months to settle. Hypoparathyroidism (lack of parathyroid function) does not usually interfere with normal daily living or work.
Wound Healing
We pay particular attention to the wound from thyroid surgery. Just like every patient is different, every scar is also different. If your neck is long and thin and the thyroid is small, then the scar is usually about 4-6 cm above the collar line. We will make the scar longer to suit the conditions we find and so that surgery can be performed safely with good vision.
Some people are prone to form a red, raised up (hypertrophic) scar. This is seen more in young people with pigmented skin. The scar usually gets better with time but may take 6 to 18 months. If a scar is particularly hypertrophic (and these can sometimes be itchy as well), we may ask a plastic surgeon to advise regarding treatment, but we usually wait 12 months before referring.
Unsatisfactory scars affect perhaps 3% of patients. Some patients have numbness in the skin above the scar. In men this can be a problem with shaving. The numbness settles after about 6 months. Some patients experience a feeling of tightness in the neck. This symptom settles in most cases over 2 weeks but may take up to 6 months to subside. There may be a feeling of difficulty swallowing during that time and sometimes pain and an irritating cough.
Patients who have a low thyroid hormone level are more prone to neck swelling and tightness and correction of the low level with thyroid hormone may help. Rarely these symptoms can be persistent, but usually not severely disabling.
Bleeding
Bleeding is an uncommon complication after thyroid surgery. Even a small amount of blood collecting around the throat (haematoma) can cause swelling and breathing problems. For this reason, we watch thyroid patients closely after their surgery to look for any signs of swelling. Occasionally patients may develop a haematoma in the wound and will need to have this evacuated in the operating room. This risk is less than 1% of all neck operations. We take particular steps during the operation and at the end to minimise the risk of bleeding.
It is important to stop aspirin, arthritis medicines and anti-platelet drugs (eg. clopidogrel) at least 7 days before surgery. Warfarin treatment needs special arrangements. New blood thinning medications (eg. Dabigatran, Rivaroxaban, Xarelto) are becoming more popular and must also be stopped prior to surgery. There are also some herbal medicines (particularly gingko biloba, fish oil) that can interfere with blood clotting.
If you are unsure, show Dr Yeung the details of any dietary supplement or natural remedies you are using. We use a variety of techniques to secure blood vessels that run to the thyroid. These include advanced heat sealing devices, surgical ties and small titanium clips. The heat sealing devices are used as much as possible as they form a secure seal on the blood vessels and do not leave any residual material. Surgical ties that are used will commonly dissolve after weeks to months. Small titanium clips are used to secure very small arteries close to the nerves and parathyroid glands without “collateral” damage to these important structures. The clips are inert, do not rust and do not set off metal detectors, and do not move or heat up in strong magnetic fields used in Magnetic Resonance Imaging (MRI).
Sometimes patients have neck X-rays after thyroid surgery and are alarmed when the report notes “surgical clips are seen in the neck” and think that instruments have been left there by mistake! These clips are used in most branches of surgery and do not produce adverse health problems.
Getting back to normal activities
Most patients recover quickly from their thyroid operation and are well enough to leave hospital on the first day after surgery. We advise taking it easy at home for about 10-14 days after thyroidectomy. Some patients who feel unable to relax, or run their own business return to work after about 5 days.
Occasionally the recovery time may be longer, for example if the voice is recovering, and we take this into consideration when providing a medical certificate. As the neck muscles may be stiff, it is important not to drive until you can turn your head comfortably to have full vision of the inside lane and when reversing. Heavy housework should be avoided for 2 weeks, and really heavy manual work and heavy lifting above shoulder height avoided for 6 weeks.
Contact sport should be avoided for 6 weeks but exercise to maintain fitness such as walking, running and cycling may be started after 7-10 days. Recommencing sexual relations is best guided by individual patient comfort levels and common sense.
Hemithyroidectomy
Hemithyroidectomy or thyroid lobectomy is where one of the thyroid lobes is removed.
Why am I having a hemithyroidectomy?
Some reasons for needing to undergo a hemithyroidectomy include:
1. Indeterminate nodule (Bethesda category 3 or 4 on biopsy)
Your biopsy shows that there is a lump within the thyroid which contains abnormal cells. About 15 – 30% of these turn out to be thyroid cancer. The other 70 – 85% contain active cells in a nodule which is growing, but which we cannot rule out being cancerous without removing the whole lump and the thyroid lobe in which it sits. Due to the result of your biopsy a definitive diagnosis can only be made after the thyroid lobe is removed and a detailed examination under a microscope of many slices from around the lump to look for cells spreading into the thyroid tissue or blood vessels. If a cancer is diagnosed, a second operation may be needed to complete the surgical treatment.
2. Non diagnostic biopsies
Fine needle thyroid biospies are normally able to make a diagnosis of whether a nodule is cancerous or not. Occasionally, particularly after 2 biopsies are perfomed, there are no cells seen in the biopsy. This is known as a non-diagnostic (Bethesda Category 1) result. This may occur in thyroid cysts which only consist of fluid and no cells are present. However, if a sold nodule returns a non-diagnostic result, the best method to make a diagnosis will be to remove the nodule.
3. There is a large thyroid nodule which is causing pressure related symptoms
Eg. difficulty swallowing, choking feelings, coughing
4. Thyroid overactivity
Where there is a nodule in one lobe which is producing excess thyroid hormone.
5. Benign thyroid conditions which, by needing repeated investigation such as needle biopsy over time, are proving a source of anxiety and inconvenience for the patient.
On very rare occasions we find another abnormal area in the neck that was not expected from the history, examination or pre-operative tests. If we feel this is a serious abnormality (specifically that there is a cancer), we prefer to deal with it at the time. This may mean removing the whole thyroid and you will need to take life-long thyroid hormone. Most patients prefer to allow me the discretion to use my best judgment in this situation, which happens in less than 1% of cases. If you do not want to place this responsibility in my hands, you should tell me before surgery.
What are the complications of hemithyroidectomy?
These are very similar to those seen in having total thyroidectomy. There are some exceptions: Thyroxine replacement. After having one lobe of the thyroid removed, the remaining half should be able to produce adequate amounts of thyroid hormone. In approximately 10 – 30% the remnant lobe is unable to do so and you may need to take Thyroxine replacement. Dr Yeung performs a thyroid blood test at approximately 3 months after surgery to check your levels. If your levels are inadequate at that time, she will likely commence you on a small dose of Thyroxine.
Parathyroid glands
As only one lobe is being removed, there should be 2 parathyroid glands on the other side which will be unaffected. Consequently there should not be any problems with a drop in the parathyroid hormone (PTH) and calcium levels. The exception to this is if you have had your other thyroid lobe removed in the past. In this case the situation following a total thyroidectomy will apply to you.
Primary hyperparathyroidism
Primary hyperparathyroidism (PHPT) is a disorder of the parathyroid glands.
What is primary hyperparathyroidism?
Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. “Primary” means this disorder originates in the parathyroids ie. one or more enlarged, overactive parathyroid glands secretes too much parathyroid hormone (PTH). In secondary hyperparathyroidism, a problem such as kidney failure causes the parathyroids to be overactive.
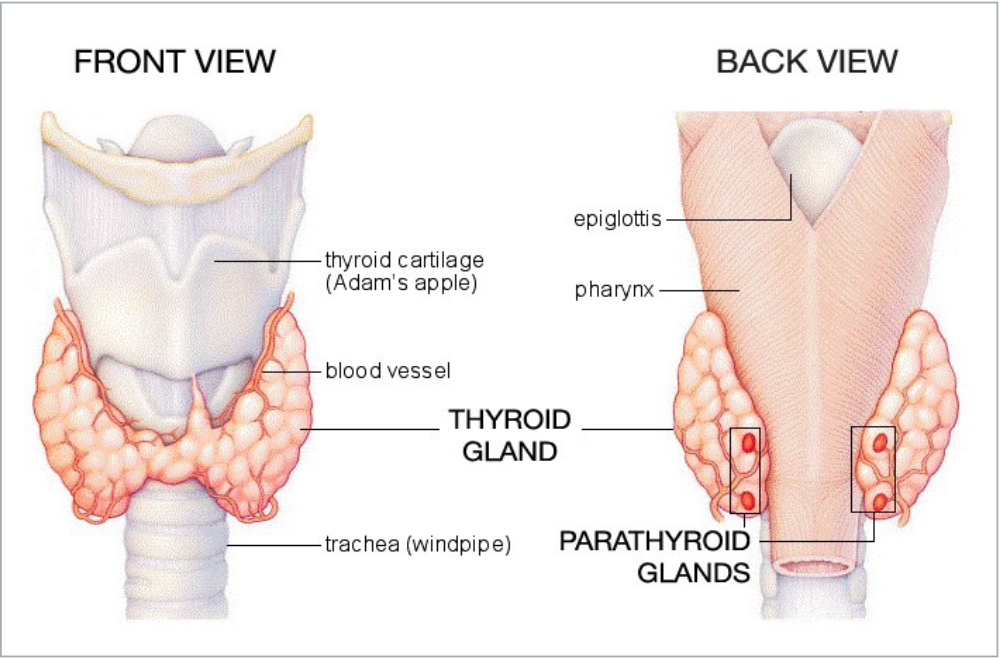
What are the parathyroid glands?
The parathyroid glands are four tiny glands located on the back of the thyroid gland, in the neck (see above diagram). Though their names are similar, the thyroid and parathyroid glands are entirely different glands, each producing distinct hormones with specific functions. The parathyroid glands secrete parathyroid hormone (PTH), a substance that helps maintain the correct balance of calcium and phosphorus in the body. PTH regulates the level of calcium in the blood, release of calcium from bone, absorption of calcium in the intestine, and excretion of calcium in the urine. When the level of calcium in the blood falls too low, the parathyroid glands secrete just enough PTH to restore the blood calcium level.
What is hyperparathyroidism?
If the parathyroid glands secrete too much hormone, as happens in primary hyperparathyroidism, the balance is disrupted, leading to a rise in blood calcium. This condition of excessive calcium in the blood, called hypercalcaemia, is what usually signals the doctor that something may be wrong with the parathyroid glands. In approximately 85% of people with primary hyperparathyroidism, a benign tumor called an adenoma has formed on one of the parathyroid glands, causing it to become overactive. Benign tumors are noncancerous.
In most other cases, the excess hormone comes from two or more enlarged parathyroid glands, a condition called hyperplasia. Very rarely (<1%), hyperparathyroidism is caused by cancer of a parathyroid gland. This excess PTH triggers the release of too much calcium into the bloodstream. The bones may lose calcium, and too much calcium may be absorbed from food. The levels of calcium may increase in the urine, causing kidney stones. PTH also lowers blood phosphorus levels by increasing excretion of phosphorus in the urine.
Why are calcium and phosphorus so important?
Calcium is essential for good health. It plays an important role in bone and tooth development and in maintaining bone strength. Calcium is also important in nerve transmission and muscle contraction. Phosphorus is found in all bodily tissue. It is a main part of every cell with many roles in each. Combined with calcium, phosphorus gives strength and rigidity to your bones and teeth.
What causes hyperparathyroidism?
In most cases, we don’t know the cause. The vast majority of cases occur in people with no family history of the disorder. Only about 5 percent of cases can be linked to an inherited problem. Familial multiple endocrine neoplasia (MEN) type 1 is a rare, inherited syndrome that affects the parathyroids as well as the pancreas and the pituitary gland. Another rare genetic disorder, familial hypocalciuric hypercalcaemia (FHH), is sometimes confused with typical hyperparathyroidism. Each accounts for about 2 percent of primary hyperparathyroidism cases.
How common is hyperparathyroidism?
In the United States, about 100,000 people develop the disorder each year. Women outnumber men two to one, and risk increases with age. In women 60 years and older, two out of 1,000 will develop hyperparathyroidism each year. Australian data is not available, however is estimated to affect around 1% of the population.
How is hyperparathyroidism diagnosed?
Hyperparathyroidism is diagnosed when tests show that blood levels of both calcium and parathyroid hormone are too high. Other diseases can cause high blood calcium levels, but only in hyperparathyroidism is the elevated calcium the result of too much parathyroid hormone. A blood test that accurately measures the amount of parathyroid hormone has simplified the diagnosis of hyperparathyroidism. Once the diagnosis is established, other tests may be done to assess complications. Because high PTH levels can cause bones to weaken from calcium loss, a measurement of bone density can help assess bone loss and the risk of fractures. A 24-hour urine collection may provide information on kidney damage, the risk of stone formation, and the risk of familial hypocalciuric hypercalcemia.
How is hyperparathyroidism treated?
Surgery to remove the enlarged gland (or glands) is the main treatment for the disorder and cures it in 95 percent of operations. Calcimimetics are a new class of drug that turns off secretion of PTH. They have been approved by the Food and Drug Administration for the treatment of hyperparathyroidism secondary to kidney failure with dialysis, and primary hyperparathyroidism caused by parathyroid cancer. They have not been approved for primary hyperparathyroidism, but some physicians have begun prescribing calcimimetics for some patients with this condition. Patients can discuss this class of drug in more detail with their Endocrinologist.
Are there any complications associated with parathyroid surgery?
Surgery for hyperparathyroidism is highly successful with a low complication rate when performed by Endocrine Surgeon. About 1 percent of patients undergoing surgery may experience damage to the nerves controlling the vocal cords, which can affect speech. One to 5 percent of patients lose all their parathyroid tissue and thus develop chronic low calcium levels, which may require treatment with calcium or vitamin D. The complication rate is slightly higher for hyperplasia than it is for adenoma since more extensive surgery is needed.